Category:
NIHON KOHDEN (日本光電) Life Scope monitoring history from the 1990s, Life
Scope monitors networking; Nihon Kohden Life Scope BSM-8000
series bedside monitors, Life Scope S (BSS-9800) bedside station, Life Scope M (BSM-9501)
modular monitor, Life Scope J (BSM-9101) bedside monitor, Life Scope TR (BSM-6000 series) bedside monitor, Life Scope G5 (CSM-1500 series) bedside monitor, Life Scope
G7 (CSM-1700 series) bedside monitor, Life Scope G9 (CSM-1901) bedside monitor.

NIHON KOHDEN has been struggling with the disruptive digital revolution since the 1990s, first they failed to make two workable digital modular monitors and made an extremely unwise move to cover this up with being the first in the world to promote the use of flexible sockets when there was no demand in the market for socket flexibility. All of the efforts were just to avoid spending time and money to develop a digital measurement LAN network for bona fide modular monitors.
The weak financial situation led to poor internal safeguards in corporate conduct, initially exporting unproven and unapproved new-type bi-phasic defibrillators in November 2002; with passing time, subsequent events turned even more bizarre. A hidden ticking time bomb is just waiting to explode with many key issues unaddressed and buried.
(CHAPTER I)
Back To The Future In The 1990s
The longer you can look back, the farther you can look forward - Winston Churchill
| The Digital Revolution |
|---|
| dealt a heavy irrecoverable blow to NIHON KOHDEN as a manufacturer |
|---|
First, for perspective: The highest revenue for NIHON KOHDEN CORPORATION from exports comes from patient monitors, followed by defibrillators, together they formed more than 70% of the company's sales in foreign markets. All other products contribute only a small part to the export business; if your understanding is not the same, it is due to the man-made noises.
The disruptive digital revolution brutally pushed back by decades the technological progress of NIHON KOHDEN, whose strength is mainly in traditional analog electronics; many of you will be stunned to learn what is the company's current digital capability, for example, for patient monitoring. The details are available in this article for your critical evaluation.
As patient monitors is the top product category for export, we should first look at the patient monitoring range since the 1990s.
During the 1990s, the company was seen grappling with a huge technological gap to catch up with International players, with digital Ethernet networking being the norm in foreign markets while Nihon Kohden
Corporation
in Japan was still helplessly struggling with the outdated analog type signal
exchangers. The only reason the company is still around today is simply because Japanese domestic market for medical equipment is a protective one, and domestic companies are insulated from competing directly with foreign companies on the basis of technologies.

| The patient monitoring products |
|---|
| were naturally shunned in foreign markets |
|---|
The problem faced by the company in foreign markets has always been how to create value using outdated technology! The absence of know-how to offer even basic level of digital networking (LAN) in
Patient Monitors in the 1990s meant
the collapse of NIHON KOHDEN export sales for Life Scope Patient
Monitors; the only exception was export sales linked to Japanese Government ODA projects. As seen in the USA
market, sales recovery was so gradual and hardly noticeable that many
from the
younger generation had erroneously mistaken it as a new
emerging brand in the market!
For a
good SUMMARY of the Patient Monitoring market up to the late 1980s,
Michael E. Porter had one in his book The Competitive Advantage of Nations (1990; Republished with a new introduction, 1998).
| The types of products the company |
|---|
| was exporting in 1997 |
|---|
Take a look at this scanned copy of the Nihon Kohden 1997 Product Guide (click for PDF),
the booklet contained the details of CardioLife TEC-2200 series
defibrillators which were officially launched in May 1997, thus May 1997
sets the earliest possible publication date of this product guide beyond the
slightest doubt.
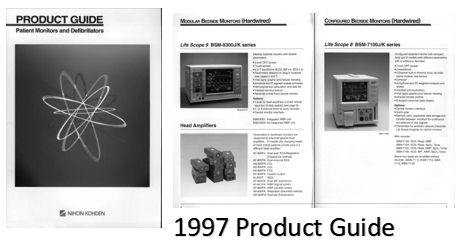
The patient monitors in the said guide show product details of Life Scope 9, Life Scope 14, Life Scope LC etc. linking to CNS-8300 Central Monitors via bulky analog signal exchangers instead of compact digital network hubs.
Information about USA
FDA registrations during this period for Nihon Kohden patient monitoring products are readily accessible on the Internet.
 |
| The legacy analog signal exchange network was the only type available for sales in 1997 |